67YR OLD WITH SOB, BILATERAL PEDAL EDEMA AND LOW BACKACHE
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
PREFINAL CASE REPORT:
Shortness of breath since 2 months



PROVISIONAL DIAGNOSIS : COPD WITH RIGHT HEART FAILURE and BACKACHE (under evaluation)








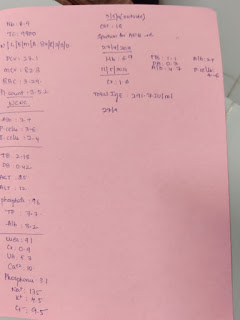
Above Investigatons:-
Ph-7.4
Pco2- 43.3
Po2-97.4
SPo2-95
Hco3-26.7
On 4 ltrs o2
Blood group-A positive
RBS- 132 mg/dl
Blood urea- 50mg/dl
Hemogram:
Hb - 11 gm/dl
TLC - 12400
N/L/E/M-92/3/2/3
PCV-36.2.2
MCV-75.9.9
MCH-23.1
MCHC-30.4
RDW - CV-17.4
PLT- 2.30
NC/NC with neutrophilic leucocytosis
Phosphorous-3.6 mg/dl
Serum ca+2 - 9.2 mg/dl
Serum creatinine- 0.9
LFT:
Tb - 1.71
Db- 0.50
SGOT(AST) - 41
SGPT(ALT) - 38
ALP-250
Tp-5.4
Albumin-2.98
A/G - 1.23
SERUM ELECTROLYTES:
Na+ - 141
K+ - 4.3
Cl - - 97










USG:











SOAP UPDATES
27/3/22
S-C/o SOB
PEDAL EDEMA DECREASED
O-
O/E:No pallor/Icterus/Cyanosis/Clubbing/Generalised Lymphadenopathy.
Temp:Afebrile
PR:96bpm
BP:110/70 mm of hg
RR-18
SPO2-99%@10L O2
CVS:S1,S2 heard,no murmurs
RS:BAE+,NVBS heard on left side and on right side wheeze and crepts are present .
P/A:SOFT,NON TENDER,BS+
CNS-PT CONSCIOUS,SPEECH NORMAL
CRANIAL NERVES-NORMAL
REFLEXES-
RT. LFT
BICEPS-. 1+. 1+
TRICEPS-. 1+. 1+
SUPINATOR- 1+. 1+
ANKLE. -. 1+. 1+
KNEE-. 1+ 1+
PROVISIONAL DIAGNOSIS:-COPD WITH RT HEART FAILURE WITH SEVERE LOW BACKACHE UNDER EVALUATION
P-
1.NEBULISATION WITH IPRAVENT AND BUDECORT-8th HOURLY
2.INJ LASIX 40 MG IV/BD
CHECK BP BEFORE GIVING LASIX
3.STRICT I/O CHARTING
4.VITALS MONITORING EVERY 4TH HOURLY
5.TAB DOLO -650 MG /PO/SOS
6.TAB HYDRALAZINE 12.5 MG PO/BD
7.TAB CARVEDILOL 3.125 MG PO
8.TAB ECOSPRIN -AV(75/20. MG) x PO/OD
9.INTERMITTENT CPAP 4TH HOURLY
SOAP UPDATES
28/3/22
S-C/o SOB
PEDAL EDEMA DECREASED
O-
O/E:No pallor/Icterus/Cyanosis/Clubbing/Generalised Lymphadenopathy.
Temp:Afebrile
PR:114bpm
BP:100/60 mm of hg
RR-22
SPO2-99%@10L O2
CVS:S1,S2 heard,no murmurs
RS:BAE+,NVBS heard on left side and on right side wheeze and crepts are present .
P/A:SOFT,NONTENDER,BS+
CNS-PT CONSCIOUS,SPEECH NORMAL
CRANIAL NERVES-NORMAL
REFLEXES-
RT. LFT
BICEPS-. 1+. 1+
TRICEPS-. 1+. 1+
SUPINATOR- 1+. 1+
ANKLE. -. 1+. 1+
KNEE-. 1+ 1+
PROVISIONAL DIAGNOSIS:-COPD WITH RT HEART FAILURE WITH SEVERE LOW BACKACHE UNDER EVALUATION
P-
1.NEBULISATION WITH IPRAVENT AND BUDECORT-8th HOURLY
2.INJ LASIX 40 MG IV/BD
CHECK BP BEFORE GIVING LASIX
3.STRICT I/O CHARTING
4.VITALS MONITORING EVERY 4TH HOURLY
5.TAB DOLO -650 MG /PO/SOS
6.TAB HYDRALAZINE 12.5 MG PO/BD
7.TAB CARVEDILOL 3.125 MG PO
8.TAB ECOSPRIN -AV(75/20. MG) x PO/OD
9.INTERMITTENT CPAP 4TH HOURLY
SOAP UPDATES
29/3/22
S-C/o SOB
PEDAL EDEMA DECREASED
O-
O/E:No pallor/Icterus/Cyanosis/Clubbing/Generalised Lymphadenopathy.
Temp:Afebrile
PR:116bpm
BP:100/60 mm of hg
RR-18cpm
SPO2-99%@10L O2
CVS:S1,S2 heard,no murmurs
RS:BAE+,NVBS heard on left side and on right side wheeze and crepts are present .
P/A:SOFT,NONTENDER,BS+
CNS-PT CONSCIOUS,SPEECH NORMAL
CRANIAL NERVES-NORMAL
REFLEXES-
RT. LFT
BICEPS-. 1+. 1+
TRICEPS-. 1+. 1+
SUPINATOR- 1+. 1+
ANKLE. -. 1+. 1+
KNEE-. 1+ 1+
PROVISIONAL DIAGNOSIS:-COPD WITH RT HEART FAILURE WITH SEVERE LOW BACKACHE UNDER EVALUATION
P-
1.NEBULISATION WITH IPRAVENT AND BUDECORT-8th HOURLY
2.INJ LASIX 40 MG IV/BD
CHECK BP BEFORE GIVING LASIX
3.STRICT I/O CHARTING
4.VITALS MONITORING EVERY 4TH HOURLY
5.TAB DOLO -650 MG /PO/SOS
6.TAB HYDRALAZINE 12.5 MG PO/BD
7.TAB CARVEDILOL 3.125 MG PO
8.TAB ECOSPRIN -AV(75/20. MG) x PO/OD
9.INTERMITTENT CPAP 4TH HOURLY
SOAP UPDATES
30/3/22
S-C/o SOB
PEDAL EDEMA DECREASED
Back pain not decreased
O-
O/E:No pallor/Icterus/Cyanosis/Clubbing/Generalised Lymphadenopathy.
Temp:Afebrile
PR:102bpm
BP:100/70 mm of hg
RR-15cpm
SPO2-99%@10L O2
CVS:S1,S2 heard,no murmurs
RS:BAE+,NVBS heard on left side and on right side wheeze and crepts are present .
P/A:SOFT,NONTENDER,BS+
CNS-PT CONSCIOUS,SPEECH NORMAL
CRANIAL NERVES-NORMAL
REFLEXES-
RT. LFT
BICEPS-. 1+. 1+
TRICEPS-. 1+. 1+
SUPINATOR- 1+. 1+
ANKLE. -. 1+. 1+
KNEE-. 1+ 1+
PROVISIONAL DIAGNOSIS:-COPD WITH RT HEART FAILURE WITH SEVERE LOW BACKACHE UNDER EVALUATION
P-
1.NEBULISATION WITH IPRAVENT AND BUDECORT-8th HOURLY
2.INJ LASIX 40 MG IV/BD
CHECK BP BEFORE GIVING LASIX
3.STRICT I/O CHARTING
4.VITALS MONITORING EVERY 4TH HOURLY
5.TAB DOLO -650 MG /PO/SOS
6.TAB HYDRALAZINE 12.5 MG PO/BD
7.TAB CARVEDILOL 3.125 MG PO
8.TAB ECOSPRIN -AV(75/20. MG) x PO/OD
9.INTERMITTENT CPAP 4TH HOURLY
S-C/o SOB
PEDAL EDEMA DECREASED
Back pain not decreased
O-
O/E:No pallor/Icterus/Cyanosis/Clubbing/Generalised Lymphadenopathy.
Vitals:
Temp:Afebrile
PR:102bpm
BP:100/70 mm of hg
RR-15cpm
SPO2-99%@10L O2
CVS:S1,S2 heard,no murmurs
RS:BAE+,NVBS heard on left side and on right side wheeze and crepts are present .
P/A:SOFT,NONTENDER,BS+
CNS-PT CONSCIOUS,SPEECH NORMAL
CRANIAL NERVES-NORMAL
REFLEXES-
RT. LFT
BICEPS-. 1+. 1+
TRICEPS-. 1+. 1+
SUPINATOR- 1+. 1+
ANKLE. -. 1+. 1+
KNEE-. 1+ 1+
PROVISIONAL DIAGNOSIS:
COPD WITH RT HEART FAILURE WITH SEVERE LOW BACKACHE UNDER EVALUATION
Inj Lasix 40mg IV BD (8am-4pm)
(Check B.P before giving lasix)
Tab Hydralazine 12.5mg PO/BD
Tab Ecosporin AV/75/20mgPO/OD
Tab Ultracet 1/2 tab QID
Intermittent CPAP for 4 hours (With gap of 2hrs during feeds)
Vitals monitoring every hourly
Inj Zolendronic acid 4mg IV STAT

Comments
Post a Comment