38yrs old with renal calculi with aki and gross hydronephrosis
CASE :
38 yr old male patient came to medicine opd with chief complaints of
1. Decreased appetite since 3months
2. Fever 3months ago which lasted for 10 days
History of presenting illness :
Patient was apparently asymptomatic 3months back then he developed fever which is insidious in onset and lasted for 10 days
Fever was low grade fever and intermittent. Relieved on medication. Associated with nausea. Not associated with headache,cold, cough.
Then he developed Loss of appetite since 3months. He visited Rmp initially for loss of appetite and used medication for a month but it did not subside.
Then he went to mbbs doctor and got tests and scan done and found out that his serum creatinine level was 6mg/dl. He got his creatinine levels checked again after 15 days and found it out to be 16mg/dl . At the time of admission in our hospital his creatinine level was 20mg/dl.
On ultrasound scan done outside he was found out to have bilateral ureteric obstruction ( calculus) and hydronephrosis.
No history of pain abdomen, back ache, burning micturition and decreased urine output.
He underwent dialysis in our hospital two times.
PAST HISTORY :
No similar complaints in the past.
Patient is not a known case of diabetes mellitus, hypertension, Tb, Asthma, Cad.
PERSONAL HISTORY :
DIET : mixed
APPETITE : Decreased appetite
SLEEP : Adequate
BOWEL AND BLADDER : Constipation
ADDICTIONS : Smoking : 2 packs Beedi per day
Alcohol : consumes around 90ml - 3 times in a week.
ALLERGIES : No food and drug allergies.
FAMILY HISTORY :
No similar complaints in the family.
GENERAL EXAMINATION :
Patient is conscious coherent and cooperative.
VITALS :
Temp : Afebrile
BP : 120/70mmHg
PR : 90bpm
RR : 20 cycles/min
SpO2 : 98%
NO SIGNS OF Pallor, Icterus, Cyanosis, Clubbing,
Clubbing, Lymphadenopathy and Edema.
SYSTEMIC EXAMINATION :
CVS : S1 and S2 heard. No murmurs
RESPIRATORY : BAE + No added sounds.
P/A : Soft , non tender and no evidence of organomegaly.
CNS : No neurological deficits
PROVISIONAL DIAGNOSIS :
Acute kidney injury on Chronic kidney disease.2° to Post renal pathology and ureteric calculi with gross hydronephrosis.
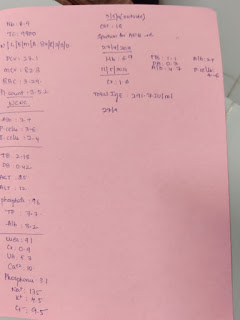
INVESTIGATIONS :
Outside : 04/10/21
USG ABDOMEN :


08/10/21
ULTRASOUND :

ECG :










11/10/21

TREATMENT :
1. Inj Lasix 40mg i.v O.D
2. Tab Nodosis 500mg b.d
3. Tab shelcal po/od
4. Tab orofor Xt Po/bd
5. Inj. Erythropoeitin 4000IU sc weekly once
6. Inj. Iron sucrose 1 ampule in 100ml ns i.v over 30mins weekly once
7. Strict bp and pr monitoring 4hrly
8. Syrup

Comments
Post a Comment